A NEXT STEP, IF YOU'RE READY
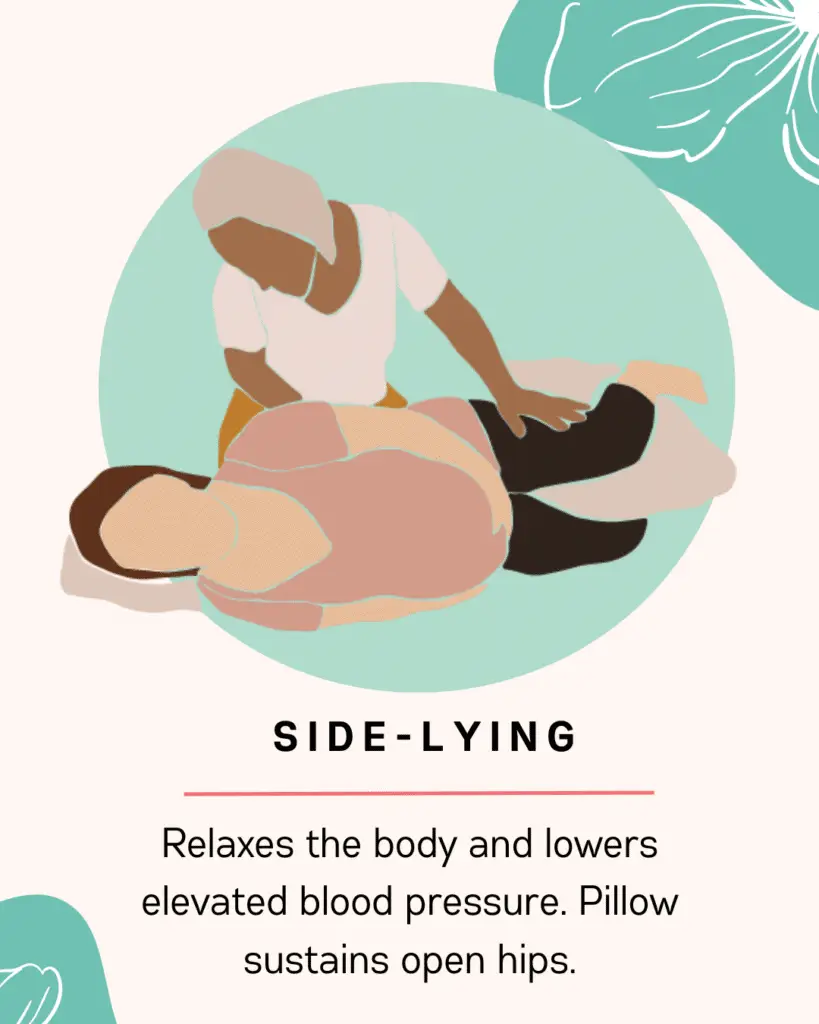
Practice these positions before labor starts.
Our birth prep course walks you through pushing positions, labor coping, partner support, and the advocacy scripts you'll want in the room. So you walk in grounded, not guessing.
Explore the course
→